Chiari Malformation
What is a Chiari malformation?
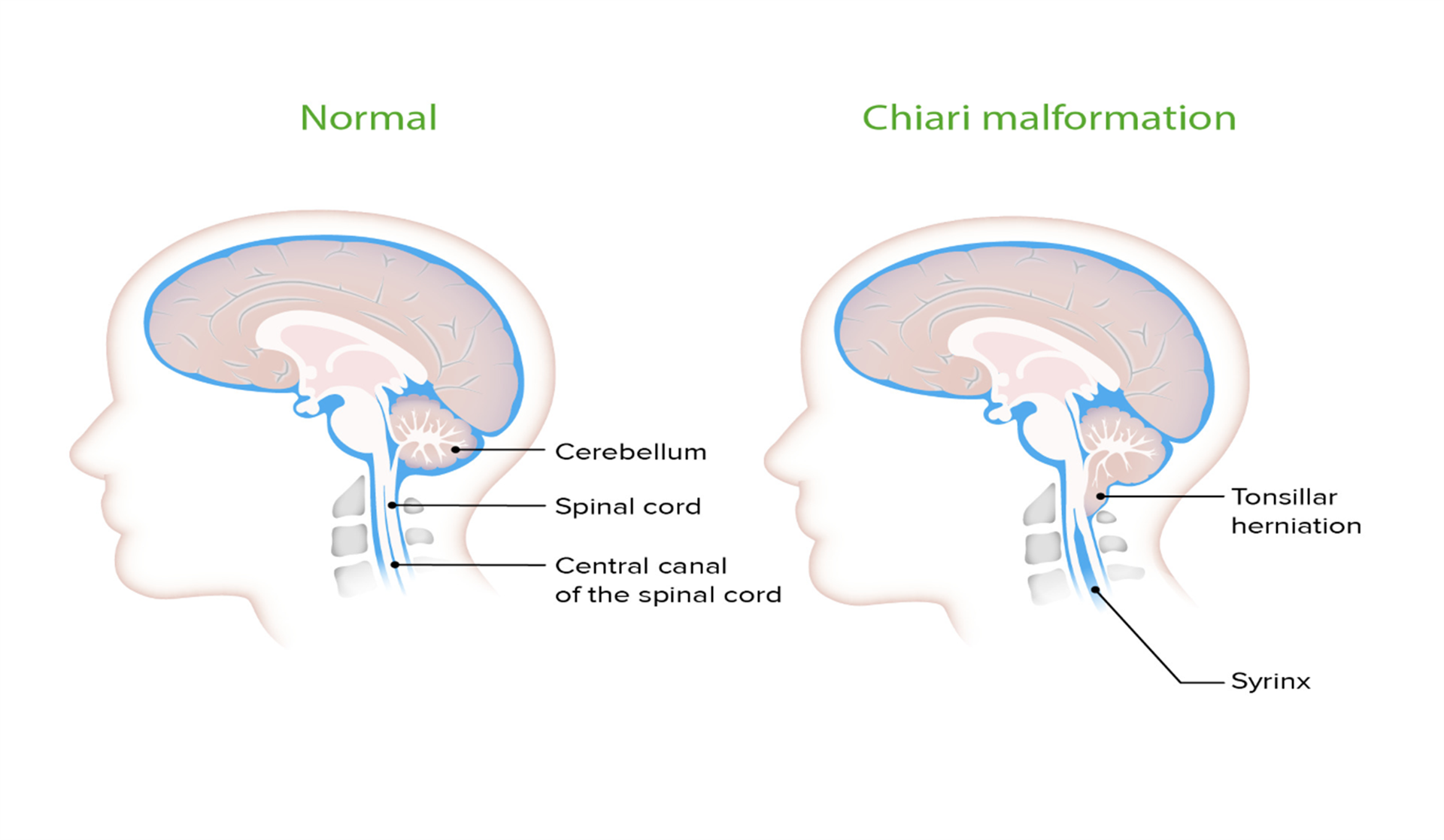
A Chiari Malformation (Hindbrain hernia) is a developmental abnormality which affects the cerebellum. This part of the brain lies at the back of the head, low down and at the top of the spinal canal. The cerebellum is divided into different parts, and the lowest tips are called tonsils.
These tonsils have no function within the brain. In Chiari malformation (Hindbrain hernia), these tonsils “drop down” through the hole in the base of the skull which is called the foramen magnum. This structure is funnel like, so becomes blocked by the hindbrain hernia, as it normally only allows the spinal cord to pass through. When the tonsils “plug” the hole (foramen magnum), the fluid which surrounds your brain and spinal cord is unable to flow freely. The resulting pressure may affect functions controlled by the cerebellum and also block the flow of the cerebrospinal fluid (CSF), the clear liquid which surrounds the brain and spinal cord, to and from the brain.
Types of Malformation
There are four types of malformation, with Type I and II being the most common.
TYPE I involves the extension of the cerebellar tonsils, without involving the brainstem,
usually first noticed in adolescent hood or early adulthood. It is the only one which can be acquired
TYPE II involves the cerebellar tonsils and the brainstem tissue into the foramen magnum. Type II is often associated with Spina Bifida due to general disruption of the development of the brain and spinal cord.
Types III and IV are rare , and although described in text books, they are not commonly seen in clinical practice.
What does a Hindbrain hernia cause?
Hindbrain hernias tend to cause headache, pain at the back of the neck and head.
This is often made worse on coughing, straining or sneezing. There may be symptoms
of visual disturbance /blurred vision, problems with balance and coordination, unsteadiness, problems with swallowing or voice, “funny turns” and possibly some altered sensation to the hands, arms and legs.
How is it diagnosed?
Your doctor will make the diagnosis from the symptoms you have , then you will undergo further testing. This may include X-rays, CT scans or MRI scans. This will give the neurosurgeon detailed information, which they will then discuss with you.
How is it treated?
If your consultant has diagnosed you with a hindbrain hernia (Chiari malformation), this doesn’t necessarily always mean you need to have surgery. This may only be indicated if the condition poses a threat to your life, or with serious disability. If your consultant is concerned that your symptoms are significantly affecting your quality of life, or your symptoms become increasingly distressing, then they may discuss surgery with you.
You must decide in this instance if your symptoms are so bad you would consider surgery. The treatment, if successful , may resolve the headaches but should be seen as a procedure to prevent worsening of your neurological symptoms. Pain, limb weakness and sensory symptoms may not respond as well. Your neurosurgeon will discuss this with you. Also, more than one surgery may be required to treat the condition.
Conservative management
There are times when it is feasible to offer you non surgical management (conservative management). This is often the case in uncomplicated hindbrain her-nias. Your neurosurgeon will arrange regular follow up appointments and scans, with the option of surgery if your condition worsens.
What does surgery involve?
Your operation will involve an incision at the base of your skull, where your head joins to your neck, and the removal of a small portion of the bone which makes up the funnel, to make it larger. The Dura (the covering of the brain and spinal cord) may need to be opened and the neurosurgeon may then shrink the cerebellar ton-sils if required. This will be determined on an individual basis and discussed with you by your neurosurgeon.
The surgery aims to relieve the pressure on the cerebellum and enable the brain and spinal fluid to flow effectively.
Risks of surgery
All risks will be discussed with you prior to your surgery. Although they are not common, you should be aware that there is potential for them to occur.
- Risks of anaesthesia
- Risk of injury to the nerves or spinal cord causing weakness/ numbness/pain
- Risk of stroke
- Risk of swallowing problems due to bruising, swelling or damage to the nerves.
- Voice hoarseness/vocal cord problems.
- Risk of leakage of the fluid which surrounds the brain and spinal cord (CSF).
- Risk of infection, which includes MRSA and Menigitis
- Bleeding or haematoma( collection of blood under the skin).
- Risk of developing hydrocephalus (an excessive build up of CSF in the brain) which may require further surgical treatment in the form of ICP monitoring, shunt, insertion of external ventricular drain or third ventriculostomy.
For any of these interventions please see separate patient information.
As mentioned, complications are rare. If you are worried about any aspect of your surgery, you will have the opportunity to discuss these prior to your surgery, following your admission to hospital.
You will have a pre operative appointment to assess if you are ft to undertake anaesthetic for your surgery. They will provide a body wash /shampoo for you to use before your admission and on the day of surgery to aid prevention of infection
Are other conditions related to Chiari malformation?
Yes there are other conditions which are often linked to Chiari Malformation. These can include;
Hydrocephalus
This is an excessive build up of CSF in the brain. A Chiari Malformation can block the flow of the fluid pathway. This can occur with any type of Chiari malformation. This would need to be treated prior to your Chiari decompression.
Syringomyelia
This is a disorder in which a CSF fluid filled tubular cyst, or syrinx, forms within the spinal canal.
Tethered cord syndrome
This occurs when the spinal cord attaches itself to the bony spine. This causes pro-gressive stretching of the spinal cord resulting in damage to the muscles and nerves in the lower body and legs.
Spinal curvature
Two types of curvature can occur in conjunction with Chiari Malformation: Scoliosis (bending of the spine to the left or the right) and Kyphosis (a forward bending of the spine).
Post Operative Advice following Chiari Decompression
Pain
You will be sore and uncomfortable post operatively. This is normal. You will be given strong analgesia to help control your pain. Please let the nurse who is looking after you know if your pain is not controlled, as alternatives will be available.
Nausea and Vomiting
You will experience some nausea and vomiting following your surgery. This is be-cause of the area of the brain involved in your surgery. Again, you will be given strong anti emetics (drugs to help with feeling sick and being sick) to help with this. You will be offered these at regular intervals throughout the days following your surgery.
This particular symptom may last for a while following your surgery, and your anti emetics can be continued by your GP. It is important you continue to take these once discharged for a further 1-2 weeks as needed.
Dizziness and Balance
After the operation it is not uncommon the feel a bit dizzy and unsteady. You may need a nurse to help your walking to begin with. This usually resolves in time. The sooner you return to moving and walking the quicker it should resolve.
If you continue to feel dizzy or unsteady a Physiotherapist can assess you and give you advice and specific exercises.
General Advice on Posture
Good posture is important as it puts minimum stress on the joints and ligaments in the spine. When sitting try and avoid slumping with the head poking forward or a slouched posture.
When standing and walking try and keep the head upright and in the middle and your shoulders relaxed.
Neck pain and stiffness
Movement will not cause any problems with the stitches or wound.
You will experience some upper neck stiffness and discomfort. However, you can move your neck, even though it may be uncomfortable.
Your neck is designed for movement and the sooner you start neck exercises the sooner your movements will improve.
Neck and shoulder exercises
Simple neck and shoulder exercises are designed to restore normal movement and confidence.
They can be started the first day after the operation. The movements can started gently and increased as you can tolerate. You can do them ‘little and often’ up to 10 times each.
Once you feel that you are moving your neck freely when looking around, reaching into cupboards and when talking to friends you can stop doing the exercises
Activity Advice
Regular exercise gives you stronger bones, develops fit and active muscles, keeps you supple and fit, makes you feel good and releases natural chemicals that reduce pain.
You can commence walking as soon as possible. Increase your activity gradually and build up your tolerance again over several days or weeks. Other exercises such as jogging, cycling, gym work should be introduced gradually as you feel comfortable.
You can return to day to day activity such as cooking, cleaning and shopping quickly, as soon as you feel comfortable.
Swimming can not be commenced until the surgical wound has completely healed
Lifting
Try and avoid strenuous lifting initially following your surgery. You can resume lifting when you feel able to do so.

General post operative information
When can I get out of bed?
We encourage people to get up and out of bed as soon as possible after surgery.
How big will my wound be?
Your wound will be approx 3-4 inches long, in the midline, at the back of your head, where your neck meets your head. The surgeon will place stitches inside the wound to close the deep tissues. These absorb by themselves over time.
The skin may be closed with non absorbable stitches or metal clips, which are usu-ally removed, once you are at home, after about 10 days.
Your hair will have been shaved immediately around the wound, to allow the sterile dressing to be applied post operatively. The minimum amount of hair is shaven, this will grow back quickly as your wound heals.
When can I wash my hair?
There are no set rules. You will not feel like washing your hair for the first few days after your surgery. Once you are feeling up to it, staff will assist you into the shower and provide any help you require.
If your hair is matted from your surgery, it can be washed with a special antibacterial shampoo, which will be provided for you by the staff, avoiding rubbing your wound. Once you are at home, wash your hair gently. You do not need to buy special shampoo.
How long will I be in Hospital?
This varies from person to person. Length of stay is dependant upon your previous medical history, how you recover in the immediate days post operatively, and whether you have had any post operative complications. Generally, you will be in for about 5-7 days assuming you have no complications, less if you recover quickly and longer if any complications have occurred. The total recovery period can be as extensive as 3-6months for you to be able to undertake strenuous physical activities.
Total recovery period
Recovery of lost neurological function will also vary from person to person, and it may take as long as 2 years for recovery of any lost neurological function. Beyond that period it is unlikely further improvement will occur.
How long will I be off work/college?
Decompression of a Chiari malformation is a major operation and your body will re-quire time for healing and recovery to take place. It will take AT LEAST a month or two for you to feel anywhere near to your normal self, although this can vary and take longer in some cases.
It would be advisable to expect to be away from your work/studies for at least 6 weeks perhaps as long as 3 months.
This is also dependant upon the type of work you do and how essential it is for you to return to your work. It is advisable to discuss your options with your employer or place of study prior to your surgery.
Flying
You should be feeling well enough to undertake a flight approximately 6weeks post surgery. This can be discussed directly with your neurosurgeon if necessary.
Driving
The DVLA (Driver and Vehicle Licencing Authority) do place restrictions upon driv-ing following some types of surgery. Chiari Malformation falls into the category Post Fossa Surgery and this generally does not require a set period off driving, beyond your initial recovery period.
You will require someone to collect you following your surgery, as you will not yet be recovered enough to drive yourself home.
Going Home
When going home by car you can recline the front passenger seat and adjust the head rest to support the head. This may give extra comfort.
What follow up should I expect?
Your consultant neurosurgeon will see you in clinic approximately 6-8 weeks post operatively, although this may vary slightly due to pressures on the clinic service. You will also have a check MRI scan at about three months post operatively.
If you have any problems prior to this clinic appointment, please contact your GP, who can request an earlier appointment if he/she is concerned.
If you have any of the following post discharge please contact The Walton Centre:
- Increasing headache and nausea
- Increased redness of the wound
- Clear fluid leakage from the wound
- Increased swelling of the wound
- Raised temperature with any of the above symptoms
If you are concerned about any aspect of your surgery or follow up treatment, please contact switchboard on 0151 525 3611 and ask to speak to the secretary for your consultant neurosurgeon.
Alternatively you can contact Sara Kewin Hydrocephalus Advanced Nurse Practitioner or one of the Hydrocephalus Nurse Specialist team on: 0151 525 3611
References
Chavez et al (2014 ) Comparison of operative and non-operative outcomes based on surgical selection criteria for patients with Chiari I malformations . Journal of Clinical Neuroscience Vol 21, Issue 12, December , Pages 2201-2206
Kalb et al (2012) Evaluation of operative procedures for symptomatic outcome after decompression surgery for Chiari type I malformation. Journal of Clinical Neuroscience Vol 19, Issue 9, September , Pages 1268-1272
Useful Web Sites
Ann Conroy Trust
www. annconroytrust.org 0300 111 0004
SHINE Charity
(Spina Bifida and Hydrocephalus) Information Networking and Equality
www.shinecharity.org.uk Tel 01733 555988
The Brain Charity
www.thebraincharity.org.uk Tel 0151 298 2999
- Last Updated:31 July 2023
- Review Date:31 July 2025
- Author:Sara Kewin
- Summary:
A Chiari Malformation (Hindbrain hernia) is a developmental abnormality which affects the cerebellum. This part of the brain lies at the back of the head, low down and at the top of the spinal canal.