Lumbar microdiscectomy
Admission to hospital can be a daunting experience for most people. The information enclosed in this leaflet is designed to give you information about your stay in hospital and what to expect. This information is intended to be used as a guide to your hospital experience that may vary slightly depending upon your individual requirements for further information please see patient information on British Association of Spine Surgeons website (spinesurgeons.ac.uk/Booklets)
The Walton Centre is a Regional unit that admits people 24 hours a day, 7 days a week depending upon the urgency of their condition. Although every effort is made to ensure your admission goes ahead as planned, occasionally it is necessary to cancel planned surgery at short notice.
The surgical procedure that you are to be admitted for is called a Lumbar Microdiscectomy. This is performed for someone who has a prolapsed disc in the lower back area, sometimes known as a slipped disc.
What is a prolapsed (slipped) disc?
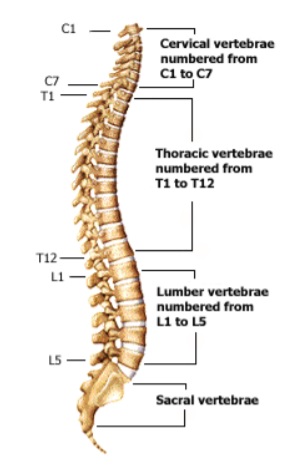
The spine is composed of small bones called vertebrae which all sit on top of each other to form your spinal column. To stop these bones from rubbing on each other you have intervertebral discs. These are soft cushions of tissue, which sit in between each of the bones in your spinal column and act as shock absorbers.
Spinal cord/Nerves
The spinal cord and nerves run through the middle of your spinal column. This acts in a similar way to a telephone exchange passing information from your brain to your body and back again. At the level of each bone (vertebra) your spinal cord sends out some nerves to transmit these messages to the body. The spinal cord finishes at the level or lumbar vertebra 1 or 2 and beyond this there is a large bundle of nerve fibres, these look very similar to a horses tail, and are called the cauda equina nerve roots. These fan out and at the level of each vertebra they send out a nerve on right and the left side.
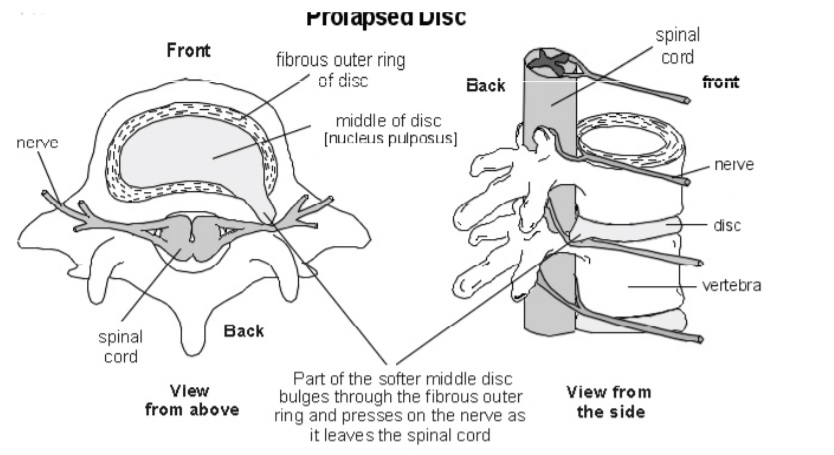
A prolapsed disc occurs when one of the cushions (discs) has a weakness at the edge and some of the internal tissue pokes out putting pressure on a nerve causing your symptoms.
What does a prolapsed disc cause?
Prolapsed discs can cause various symptoms depending on which nerves they press upon. Prolapsed discs in the lower back area cause symptoms in the legs. Usually, the pressure on the nerve causes pain to radiate down the leg and this is called sciatica. Occasionally, there may be numbness or weakness in your leg.
In a few cases the pressure can affect the nerves that supply the bladder and the bowel and this can affect the ability to pass urine and can cause numbness around the genital or anal area. In this very specific case it should be dealt with as an emergency and immediate attention is required.
Treatment
Most attacks of sciatica settle themselves after a few weeks, approx. 6-12 weeks, and will not require any surgery. The non-surgical option for treatment is to allow the body’s natural healing process to relieve the symptoms as slipped discs can resolve themselves with time relieving the pressure on the nerve. 6 out of 10 patients will feel better in 6 weeks, with 7-8 out of 10 patients better at 3 months. This can be helped by treatment from a physiotherapist, taking painkillers and keeping yourself active. In some cases osteopathic treatment or an epidural injection may also help.
If the pain does not settle spontaneously and persists with a degree of severity then surgery can be considered. The decision to proceed with surgery takes into consideration balancing the risks of surgery together with how the pain is affecting the person. Surgery allows considerable relief of pain and symptoms in 80 -90% of cases. It will, however, only relieve the leg pain and any backache will often remain. Surgery also allows the relief of symptoms earlier than if you wait for a natural recovery.
What does surgery involve?
The following information is to help you understand what we are offering you and why. Please remember, agreeing to surgery is your decision. The job of our team is to present you with the facts and options as we see them. You have the right to change your mind at any point in time, if you wish for further explanation at any time please just ask one of the staff
A microdiscectomy procedure allows the part of the disc, which is causing the pressure on the nerve, to be removed with minimal disturbance of bone and tissue. This is achieved with a microscopic surgical technique and only the piece of disc causing the pressure is removed rather than the whole disc.
Microdiscectomy involves having a small incision on the lower back whilst under general anaesthetic (You are fully asleep). A microscope is used for the surgery to give a better picture of the tissues and to minimise the disturbance to the surrounding structures, improving the accuracy. The disc is approached from behind and the fragment that is pressing on the nerve is removed, the complete disc is not excised.
What are the advantages and disadvantages of surgery?
The advantages of surgery are that there can be up to an 80-90% chance of significant relief of leg pain. However there is no guarantee that there will be any relief from back pain or an improvement in any leg weakness or changes in sensation/feeling that you may have had prior to surgery.
The risks
All the risks will be discussed with you prior to your surgery and although they are not common you should be aware that there is the potential for them to occur.
- Risk from anaesthesia
- Small risk of increased pain in back or leg, due to damage to the nerves or re-occurance of leg pain can occur because of scar tissue, nerve damage or another piece of disc moving out (6%of cases)
- Risk of injury to the nerves causing weakness or numbness in the leg this occurs in less than 1 out of 100 cases, and is more common in those having repeat surgery (10 out of 100 cases) In the extreme this can cause paralysis in the legs, difficulty with bladder/bowel/sexual function and numbness in the legs and / or the genital or anal area.
- Risk of injury to the nerves that supply the bladder, bowel and sex organs, which could result in problems with bladder, bowel and sexual function
- Leak of spinal fluid, this is were there is a tear in the lining which surrounds the nerve roots, this occurs in less than 5 in 100 patients. It is more common if you have had surgery in the same place before. This is repaired with stitches, a patch or special glue. The worst case scenario is that further surgery is required to repair the leak but this is extremely rare (0.05%)
- Risks from positioning during surgery and equipment used, this can include skin injuries, eye complications, most severely blindness but this is exceptionally rare. Special gel pads/protection are used during surgery to minimise the risk of these complications. Diathermy pads are used which is an adhesive pad placed on the skin, usually the thigh area, to minimalize heat build up, this can cause skin irritation and in exceptional and very rare cases a skin burn
- Infection, superficial wound infections can occur in approx. 4 out of 100 patients and are easily treated with antibiotics. Deep wound infections occur in less than 1 out of 100 patients, but these can require further surgery and long courses of antibiotics. Infection risk includes infection from the MRSA bacteria (infection with MRSA is very rare). Any infection can result in Sepsis but again this is exceptionally rare. Those with weakened immune systems, diabetes or taking steroid medication are more at risk of infections from surgery.
- Risk of Deep vein thrombosis (DVT, blood clot in your leg) or Pulmonary embolus (PE, blood clot in the lung). The risk is rare and we use special surgical stockings, and blood thinning injections where appropriate to reduce the risk.
- Bleeding or Haematoma, (blood clot), this can be around the wound area, and gets reabsorbed by the body over time, or in rare cases it can be within the spinal structure causing pressure to the nerve roots and requiring further surgery.
- Damage to a major blood vessel resulting in death, this is exceptionally rare (1 in 10,000 cases)
- Wound drain problems, requiring removal in theatre, whilst under anaesthetic, which again is very rare.
In 6% of patients another piece of disc at the same level can move out and cause pressure again. It is also possible for a prolapsed (slipped) disc to occur at another level in the spinal column at some time in the future.
Pre-operative assessment
It is important, if you have any changes in your pain or symptoms and also if you develop any new medical conditions or are unwell, you speak to spinal nurses or your consultants secretary at the earliest opportunity but definitely prior to attending for your admission.
In order to gain the information we need to ensure your safety during your surgery, once you have agreed to surgery you will be required to complete a pre-operative assessment online. You will be provide with the information you need on how to complete this. The information you provide will be reviewed by one of the pre op nurses. Once this is done you will be contacted to explain the next steps that will be applicable to you and the procedure you are undergoing.
For some patients you will only need to attend for some blood to be taken for testing, and routine swabs. Some patients will need to be spoken to by phone to clarify medical details, some will need to come in to clinic to be seen and examined.
It is very important that you complete your pre-operative questionnaire with all the details as accurately as possible, as inaccurate information may delay your surgery
If you do have to attend for an assessment it may include:-
1. A member of the team will discuss your medical history (your past operations and any medical conditions you may be suffering from) with you and you will be examined.
2. You may be reviewed by an Anaesthetist; he/she will have a chat with you and discuss any relevant medical history and explain what having an anaesthetic will involve.
3. You will have some blood tests performed.
4. If any x-rays or a heart trace (ECG) are required these will also be done.
5. Your medication may be prescribed; it would be helpful if you could bring with you any medication that you are taking or a list of your medication and doses. It is very important that you tell us about all your medication, including all prescribed medication, medication you buy and any herbal remedies. It is especially important that you tell us about any medication that may thin your bloods.
An appointment will be organised for you and sent to you if you are required to attend for this.
Some patients may not have a pre-operative assessment of any type, this can be for many reasons, for example, you are admitted urgently or as an emergency and there is no time for all of this to be completed. This is not a problem, because everything you need will be done the day you are admitted. Your surgery in this situation is normally the following day. You will not go home overnight.
Please be patient whilst we complete all of our assessments. It is important that we ensure everything is completed to ensure your safety. Occasionally we need to postpone surgery if your pre-operative assessment indicates that there are more tests or assessments needed before we proceed with your surgery. We understand that this is frustrating, but we will not proceed until we have all the information we require to ensure your maximum safety.
Admission to hospital
You will be able to eat and drink up to midnight the night before your surgery and drink clear water only up to 6am on the morning of your surgery. You will then be able to have sips of water only from 6am until you go for your operation. This will be clarified for you prior to your admission. Most patients will be admitted the day of their surgery at approx. 7.15, having followed the fasting instructions above.
It is advisable not to bring any valuables with you into Hospital as the Hospital does not accept any responsibility for their safety.
When you arrive you will be seen in an admission area and then informed which ward you will go to after your surgery.
The day of surgery
You will continue to be kept fasted (nothing to eat or drink) and need to wear a theatre gown, we would ask that you have a bath or shower the morning of your surgery before you leave home.
Your details will be checked with you on the ward before you go to theatre. You will be wearing a wrist band and have to answer a list of questions, for example, your name, date of birth and confirm that you have removed all jewellery, underwear and make up etc.
You will be collected for theatre and taken to the theatre reception area, where the Nurse will check you details again; whilst this can appear repetitive it is all done to ensure your safety. From there you will be taken to the anaesthetic room, where your details will be checked again. We have a robust safety check list which includes asking you to confirm what operation you are having, your symptoms, which side of the body and where you experience them, do not be concerned, this is for safety only and not because of any queries about your surgery. Once this is done the anaesthetist will give you your anaesthetic medication, and once you are asleep you will be taken into theatre and surgery performed.
The surgery will be performed by the consultant or one of his team. It is common for x-rays to be used in theatre to assist the surgeon with checking the correct position of the spinal bones and level of the spine.
After surgery you will be taken on your bed into the recovery room where you will be monitored whilst you wake up from your anaesthetic, and you will be made comfortable for your transfer back to the ward. You will be transferred back to the ward after spending approximately 1-2 hours in recovery. On return to the ward you observations i.e. blood pressure and pulse, will be checked regularly, as will your wound and your limb power and movement.
An intravenous infusion (drip) will be in your hand until you are awake enough to eat and drink again. You will be able to have sips of water a few hours after you return to the ward and then increase this as you feel well enough.
You may require a wound drain, this is a small plastic tube located just beneath the skin that comes out of the skin near wound and is attached to a plastic collection device. It drains any excess fluid/blood away from the wound but is not always needed.
If your surgery is early in the day then you should be able to get out of bed and mobilise around the ward the evening of your surgery. Once you have recovered fully from the anaesthetic we will be happy for you to be out of bed. Some patients will be able to go home the day of their surgery, if they recover quickly enough.
It is normal to feel some discomfort in the wound area after surgery and around the hip area (due to positioning in theatre) but we will manage this with appropriate pain relief medication.
If you have not been able to go home the same day as your surgery then you will go home the following day
The Day after Surgery
The day following surgery your drip will be removed, your wound will be checked and if you have a wound drain, it will be removed. Taking the wound drain out requires the nurse to remove the stitch holding it in place and gradually sliding the drain tube out. It is not normally painful and they are usually easily removed. In very rare circumstances the drain may need to be removed in theatre however this exceptionally rare.
If you have not already been out of bed you will be expected to get out of bed and move around. You may be seen by a physiotherapist if needed, however a copy of the exercises are in the back of the book to aid your recovery. You will need to bring this booklet into Hospital with you so that you will know what your exercises are and so that the Physiotherapist can complete the individual details for your exercise programme whilst explaining it to you.
One of the medical/specialist nursing team will check how you are managing. Following this you will normally be able to go home late morning or in the afternoon. It is quite normal practice to go home either the day of surgery or the day after your operation. Occasionally some patients who have had more extensive surgery may need some extra time in Hospital to recover. This is often just an extra day and is not usually more than a few extra days.
Pain medications
You may be taking 2 types of medications for pain, many patients come in for surgery having taken pain medication for a long time, such as Gabapentin, Pre gabalin, Amitriptyline, Duloxetine etc. Your doctor or specialist nurse may recommend, following your surgery, that you take a strong opioid medication alongside other painkillers such Paracetamol and your usual medication. This is to relieve the additional pain that your injuries, illness or surgery has caused.
When you are discharged, as well as your normal medication, you may be given strong opioid medication to take home. It is important that you do not exceed the maximum dose prescribed for you. It is also important that you do not take any other painkillers that have not been prescribed by the hospital at the time of your discharge. This may result in you having too much pain medicine and cause the risk of severe side effects.
If you were not already taking opioid medicines before admission to hospital, you should not need to take them for a long time. The additional pain medication, prescribed whilst you are in hospital, is only intended to be short term. As you recover and your pain reduces you will be able to slowly reduce taking the medicines.
Any medication you were taking prior to surgery should not be stopped suddenly and once you have recovered from surgery, after a few weeks, as you pain settles discuss with your GP a reducing regime for your medication You should ask you GP to review your medicines to ensure you are not taking them longer than necessary and also to ensure they are reduced safely as abrupt stopping of some medications can produce side effects.
Discharge Home
Getting home
Please arrange for a relative or friend to collect you. You will not be able to drive or use public transport. You can go home by taxi if a member of your family or friend can accompany you. If you are travelling home by car, sit in the front passenger seat and recline the seat back to make you more comfortable whilst travelling. If you cannot get transport arranged then we can arrange hospital transport, however travelling with a relative or friend would preferable if you can organise this.
Medication
Medication can be organised for you to take home, if required. Unfortunately, if we arrange medication from our pharmacy then this can mean you need to wait until later on your discharge day for it to arrive.
Sutures
Some patients will have papers stitches, or dissolvable stitches in place, some will have stitches that need removal, and some may have metal clips. Your stitches/clips will be due to be removed approximately 7 days after your surgery (in some cases longer, but this will be clarified with you before you go home). Most patients make an appointment to get this done by their GP or Practice Nurse. If you do not have access to this then a District Nurse can be organised to check your wound and remove your stitches (dissolvable stitches will only need to be trimmed at the ends) If needed then the date of your District Nurse visit will be given to you before you leave the ward. Please make sure that if you are not going home to your usual address and you are going to stay with someone else you inform the staff to ensure that the District Nurse comes to the correct address.
Wound Care
Should you have any problems with your wound after your surgery, even if your GP or District Nurse are managing this, it is very important that we are also informed as we may need to monitor your more closely. We would like you to contact us if there is any redness round the wound, wound leakage, or you have a temperature.
Please phone either:-
Spinal Nurses on 0151 556 3424
Tissue Viability Team on 0151 529 5599
You can shower, but please aim to keep the wound dressing dry, until it has healed and any sutures/clips have been removed.
Pain
It is not unusual for you to get increased pain in the leg or back, or altered sensation for a few days to a few weeks after surgery as your spinal nerves recover from your surgery. It is important that you stay mobile and continue with your physiotherapy exercises following discharge. Some patients will experience a flare up of leg pain and symptoms approx. 7 -10 days post-surgery, this usually settles over time (minimum of 6-8 weeks), but it is not unusual to get fluctuations in pain/symptoms over many weeks/months.
Activity
Remember that you have had an operation and it is usual to feel tired after this. Pace yourself and gradually build up your level of activity. Doing small things often, rather than all in one go is more sensible. It is advisable not to sit for longer than 20 mins, but to regularly get up and walk around or you will find you get stiff. You should progressively return to your normal daily routine as quickly as possible. You can undertake all the usual activities of daily life as you feel comfortable this includes walking, shopping, driving and sexual activity.
Research has shown that patients who return to normal routine as quickly as possible make the best recovery. You should progressively return to your normal daily routine as you continue to recover. You can return to work as soon as you feel you can cope even if you feel uncomfortable. Heavy lifting should only be performed in the correct way and should be avoided for the first three months.
Surgical stockings
You should wear your surgical stockings for up to 6 weeks post-surgery, if your mobility is restricted or 2 weeks if you are fully mobile to reduce the risk of DVT (blood clots in the legs), and we advise not to fly for 6 weeks post surgery, again due to the risk of DVT
Driving
You can drive when you can have a full range of movement and you must have full movement to allow you to have full control of the car, this includes being able to do an emergency stop. This is usually a few weeks after surgery.
Work
You can return to work when you feel able and this can depend on what your job role involves. Those with desk based roles may feel comfortable to return to work 4-6 weeks post surgery, but would need to be able to get up and move around to prevent stiffening in the back area. Those with more manual jobs may need to wait the full 3 months before being able to return. Please discuss this with your nurse specialist or medical team if you are unsure.
When will we see you
You will be sent an outpatient appointment for approximately 3 months following surgery by post to either come and see us, or for us to speak to you by phone, so we can check you are recovering well. Here you will be seen/spoken too by either a doctor or a nurse specialist.
Concerns
If you have any queries before then please do not hesitate to contact the spinal nurses on the advice line 0151 556 3424. Please leave you name and telephone number clearly on the answer machine so we can call you back. We try to answer the messages every working day. We work Mon- Fri 8am-6pm, we do not work weekends. We do spend a lot of time on the wards and in the out-patient clinics seeing patients, so please be patient, we will call as soon as we can.
Physiotherapy following microdiscectomy surgery
This information is intended to answer the most commonly asked questions. Any further enquiries can be directed to the Physiotherapy department.
On your first day post operatively, it is perfectly safe to:
• Be up and walking around.
• Perform daily activities such as dressing and washing.
• You may experience some hip and back discomfort; this is due to the position you were in (in theatre) and is normal. This will resolve in a few days.
• Spend time sitting out in your bedside chair, regularly changing your position is advised.
General advice
It is safe to continue with all regular activities such as cooking, cleaning, shopping and sexual activity.
You can sleep in whatever position is easiest for you.
You may continue to have some back/leg discomfort or changes in sensation especially for the first 12 weeks, this is normal.
There is no evidence to say that returning to activity and exercise leads to any adverse effects or the need for re-operation.
Symptoms to report
These are rare however if you develop any of the following symptoms you should seek medical advice without delay:
• Difficulty passing or controlling urine
• Numbness around your back passage or genitals
• Numbness, pins and needles or weakness in both legs
• Unsteadiness on your feet
Lifting
There is no restriction in bending forwards to pick up light objects or putting on your shoes and socks. We think it is sensible to avoid heavy lifting where possible to begin with. You can resume lifting when you feel able to do so. There is no given weight we advise as everyone has their own usual capabilities. You can gradually increase the amount you do until you are back to your typical ability.
Driving
You can return to driving as soon as you can sit comfortably, perform an emergency stop and that you feel safe to do so. This is a self-certification.
Work
Returning to work and normal activities will help your recovery and you should aim to do this as soon as possible. People who return to work sooner have been shown to have better outcomes. You can return to work as soon as you feel you can cope, even if your back is still uncomfortable. You may wish to grade your return to work. It may take slightly longer to be able to return to a more ‘manually heavy’ job, this can be discussed with the relevant staff members. It is normal to feel tired when returning to work after a period of sickness absence. You should plan to pace yourself and take regular breaks.
Exercise
General activity and exercise has been shown to be safe in this patient group and indeed is beneficial for your overall health. We have included an exercise programme however general activities that you may already enjoy have been proven to be as effective therefore you should look to gradually resume these. For example, hiking, swimming, cycling, jogging, yoga and pilates. Keeping a record/ diary may help you in guiding your progression. Some discomfort is normal when re-commencing activity; you should work within reasonable limits. Lower intensity exercise should be started first progressing to higher intensity over a period of weeks.
You can also safely return to recreational sports such as football or golf in a gradual manner. For specific advice with regards to contact sports/ extremes of exercise this should be discussed with your medical team.
Physiotherapy following surgery
This information has been designed for post-operative back care. It is intended to answer the most commonly asked questions. Some patients may not need physiotherapy. Any further enquiries should be directed to your physiotherapist. You may see the physiotherapist the day after your operation, or you may attend a physiotherapy group the day before or after your surgery.
Exercise programme
Exercises to be completed in sets of 10, 1 - 2 times each day. These exercises can be complemented by activities such as swimming, yoga, pilates and any other activity which you normally enjoy.
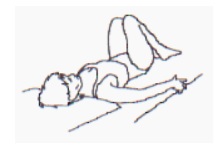
START POSITION: Lying on your back with both legs bent and your knees together.
ACTION: Slowly roll your knees from side to side keeping your upper trunk still.
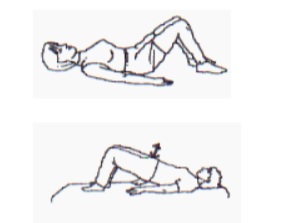
START POSITION: Lying on your back with knees bent feet on firm surface (bed/floor).
ACTION: Pull pelvic floor muscles in and lift your bottom off the bed. Hold for 10 seconds then relax. Repeat exercise 10 times.
START POSITION: Lying on your back.
ACTION: Bend the leg to be stretched forward towards your chest and hold with both arms. Hug both knees to chest. You should feel the stretching on the back of your thighs and buttock. Hold 10 seconds, repeat 10 times.

START POSITION: Lie on the back with both legs straight. Bend one hip to 90 degrees and hold the thigh.
ACTION: Hold 10 seconds then relax. Repeat 10 times. Holding the thigh in position, slowly straighten the knee until a stretch is felt at the back of the thigh. Hold 10 seconds then relax. Repeat 10 times.

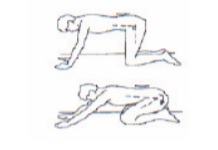
START POSITION: On hands and knees with the knees under the hips and the back relaxed in a neutral position. (Feet relaxed).
ACTION: Suck in your tummy muscles and keeping the back flat slowly rock backwards moving at the hips. Do not let the back bend or arch. Move back towards the heels until you feel the pelvis start to give. ONLY move backwards as far as the controlled flat back allows. Move slowly and do not stretch. This exercise may not be suitable for people with existing hip or knee problems.
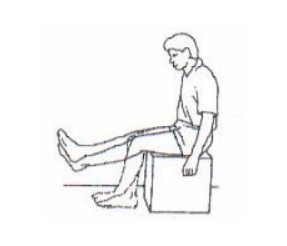
START POSITION: Sit upright with your legs side by side.
ACTION: Alternately straighten your legs and then bend each leg allowing them to swing. Do not do so much as to make it painful.
These exercises have been taken from Kinetic Control UK, with the kind permission of Mark Comerford MCSP, B.Phty., MAPA.
Preventing recurrences
- It’s your back! Maintain your good posture in sitting and standing.
- It’s your back! Immobility leads to pain, to more immobility, to more pain; hurt does not mean harm, so continue with your exercises.
- Live life as normally as possible, keep up daily activities, and try to stay fit.
- Be patient. It is normal to get aches or twinges for a time.
The information contained in this booklet is a guide to help you understand what a microdiscectomy is and what to expect. It may be that in order to address individual needs your experience is slightly different from that described.
If you have any queries, before or after, your surgery please feel free to contact us:
- Spinal Nurses 0151 556 3424
- Physiotherapy team 0151 529 5451
- Secretary to your consultant via hospital switchboard on 0151 525 3611
Visit www.thewaltoncentre.nhs.uk alternatively, log on to: www.thebraincharity.org.uk or call 0151 298 2999 for advice and information for people with neurological conditions and their carers.
- Last Updated:29 February 2024
- Review Date:29 February 2028
- Author:Spinal nurses
- Summary:
A lumbar microdiscectomy is performed for someone who has a prolapsed disc in the lower back area, sometimes known as a slipped disc.